interscalene nerve block © 2012 by Arun Nagdev is licensed under CC BY-NC-ND 4.0
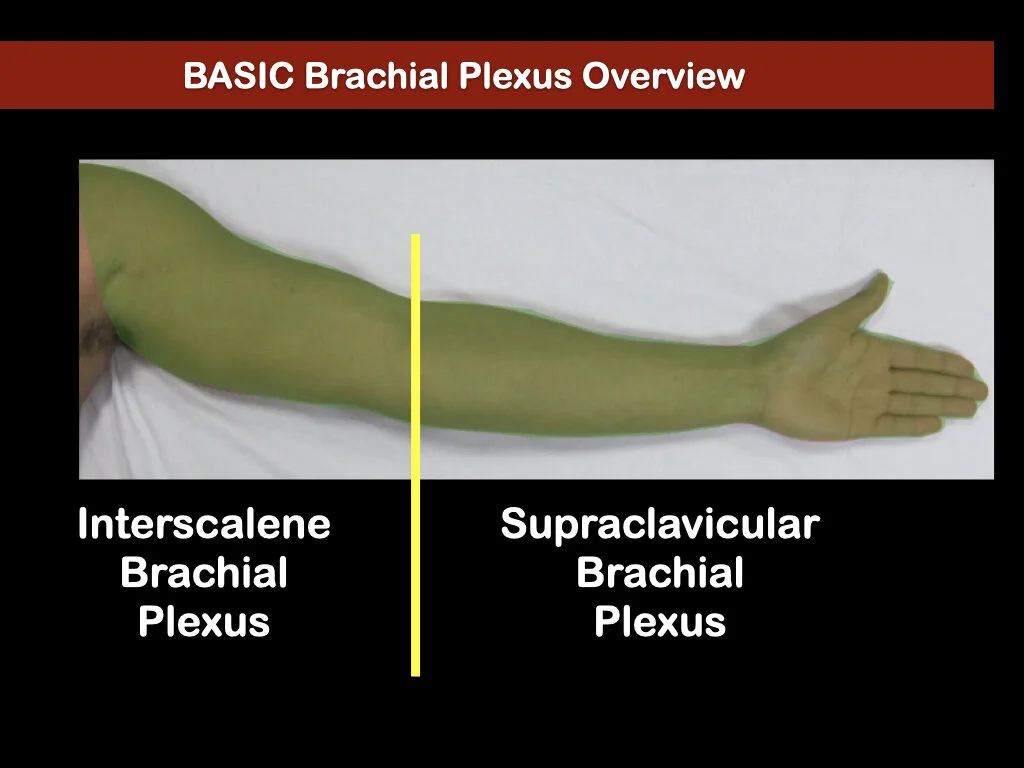
Basic Overview when thinking about Brachial Plexus Blocks
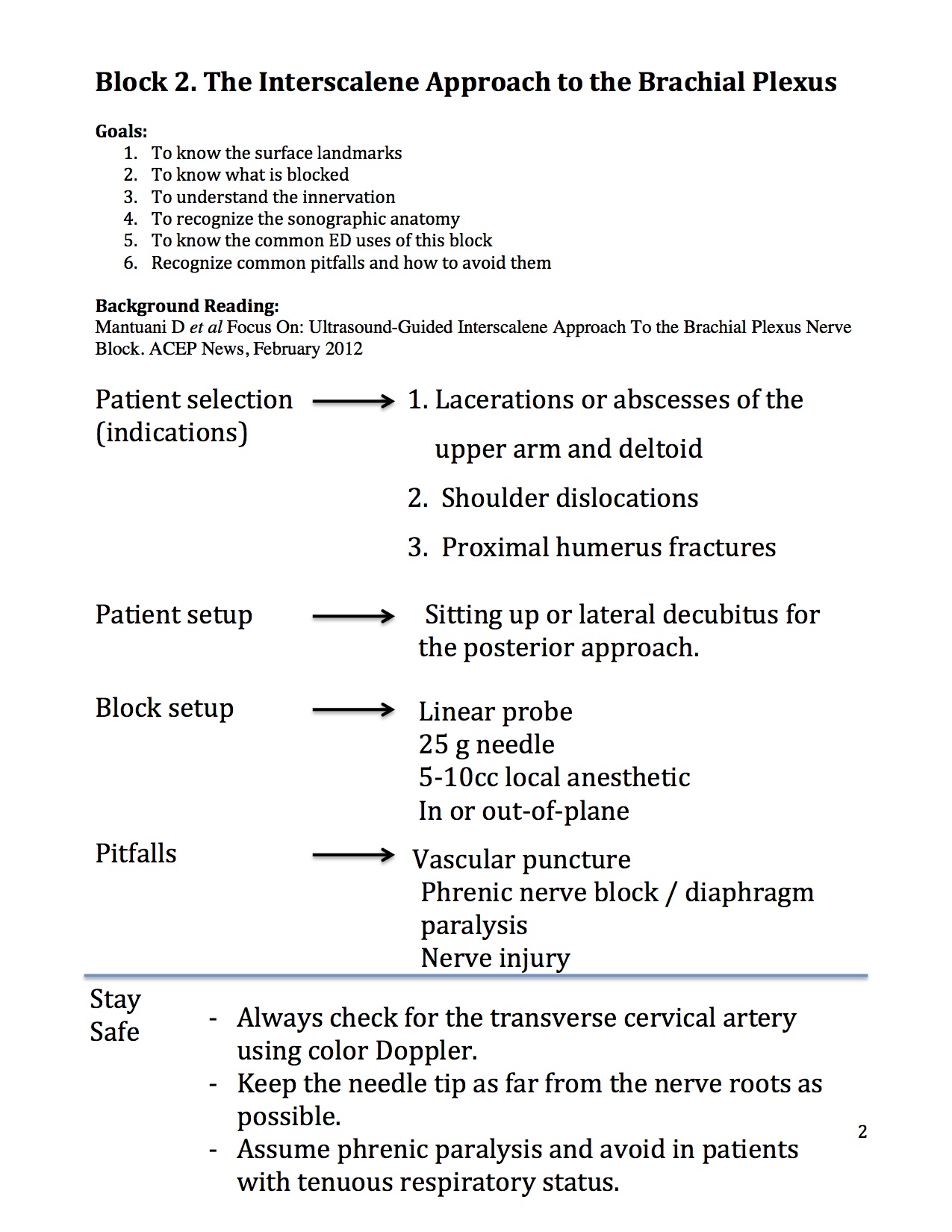
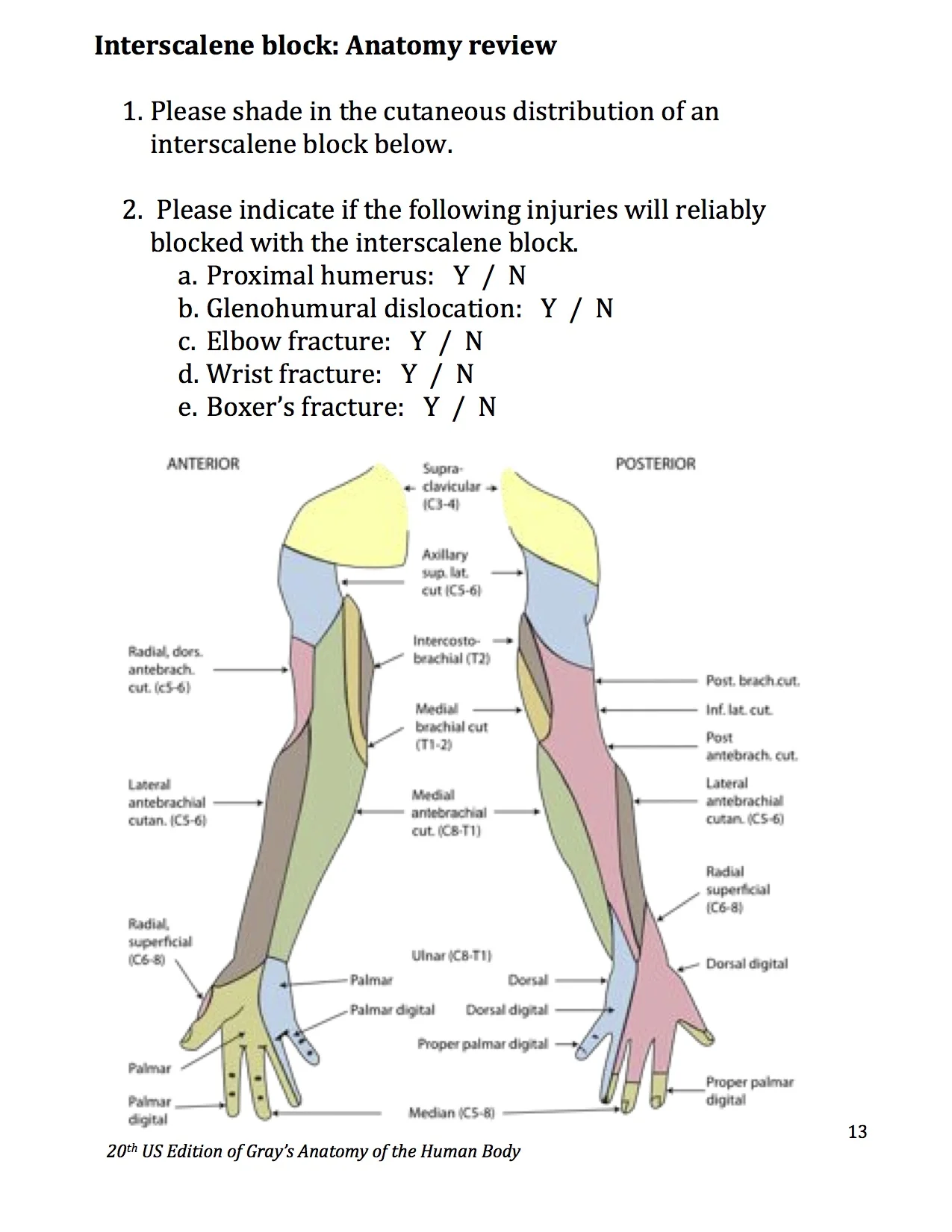
Interscalene ED Indications = humeral head/shaft fx, shoulder dislocation, deltoid abscess, etc.

Blunt tip block needle recommended

Roll the patient so he/she can see the ultrasound screen

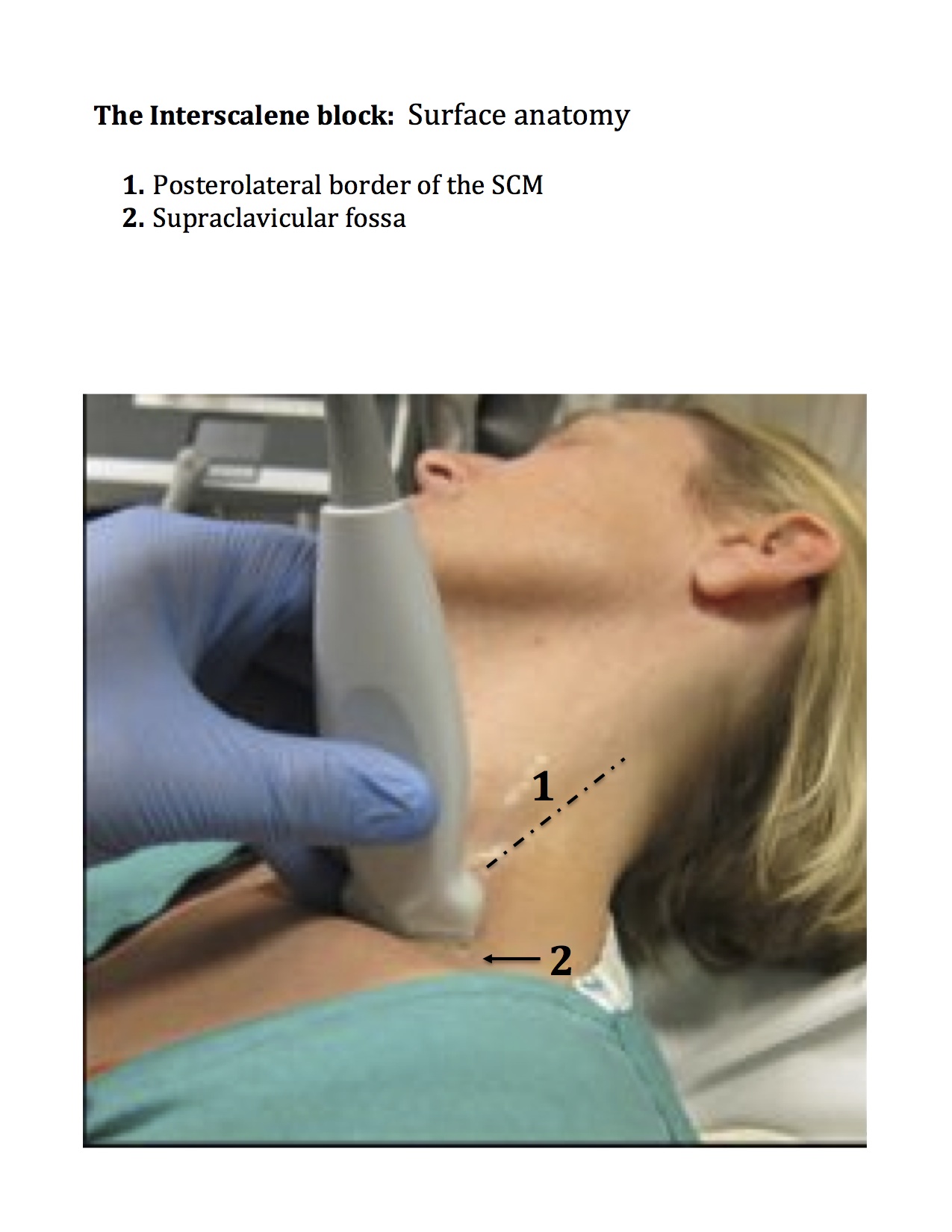
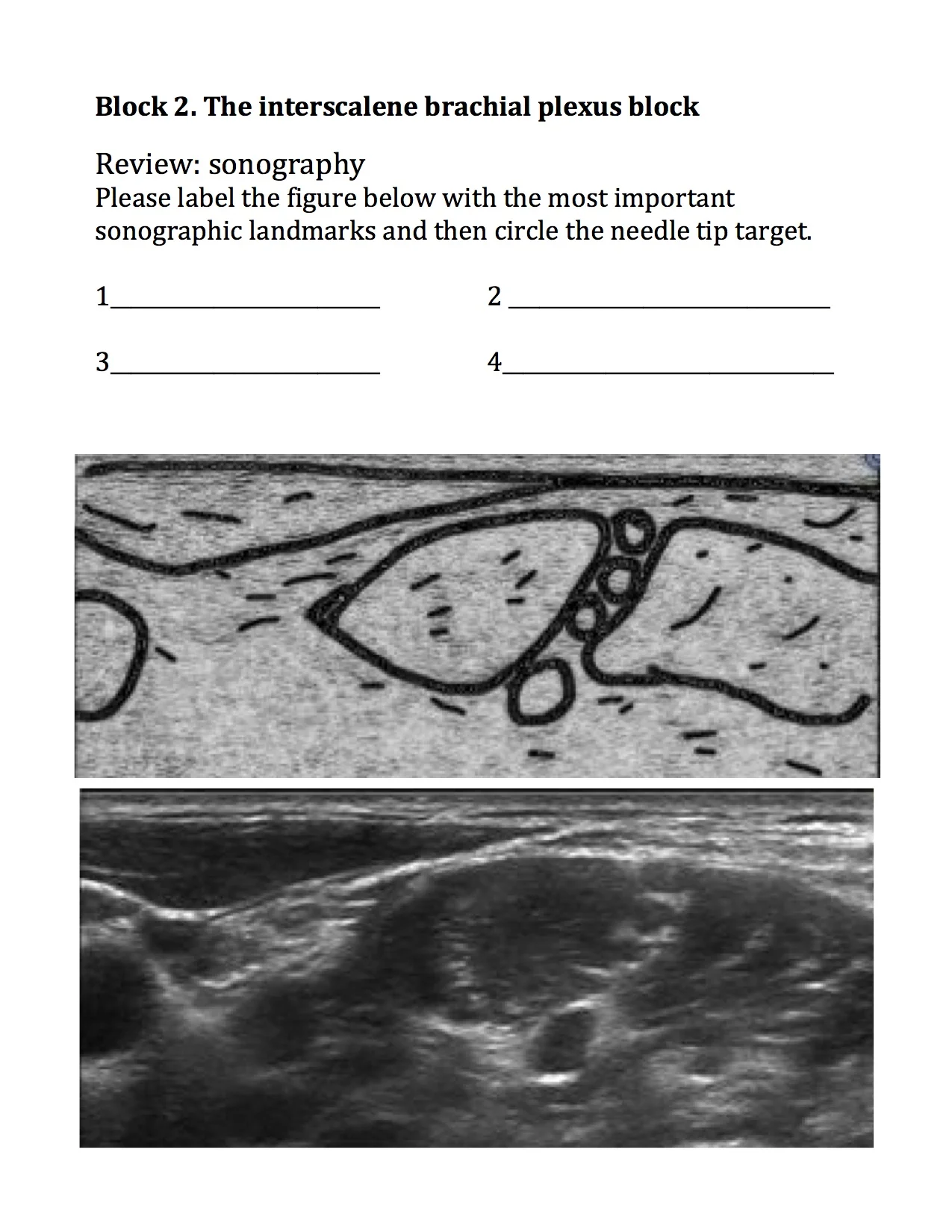
Classic way to find the interscalene brachial plexus, but often difficult for novice sonographers or in patients with atypical anatomy.

Can also do the “track back” technique by locating the Supraclavicular brachial plexus and following it back up to the Interscalene location.

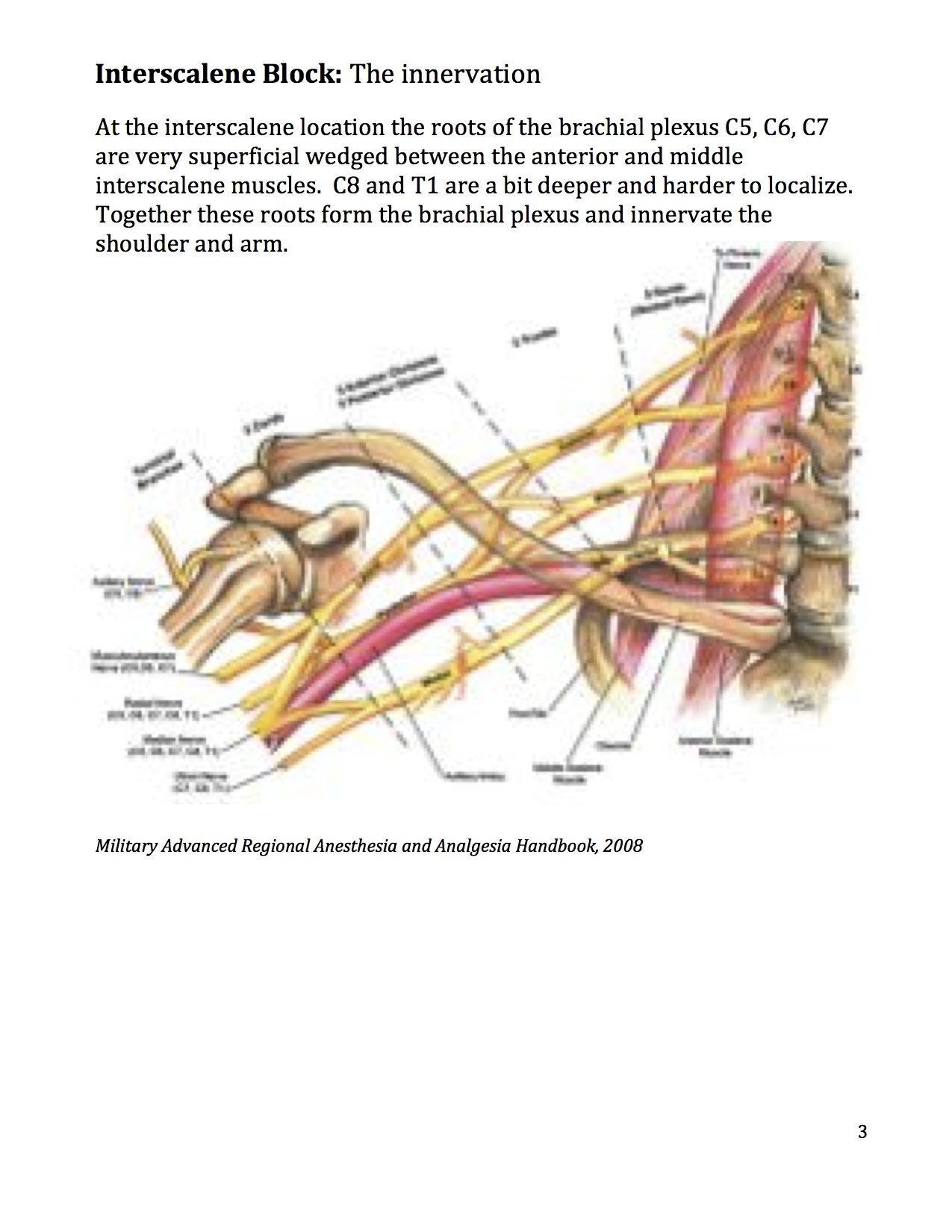
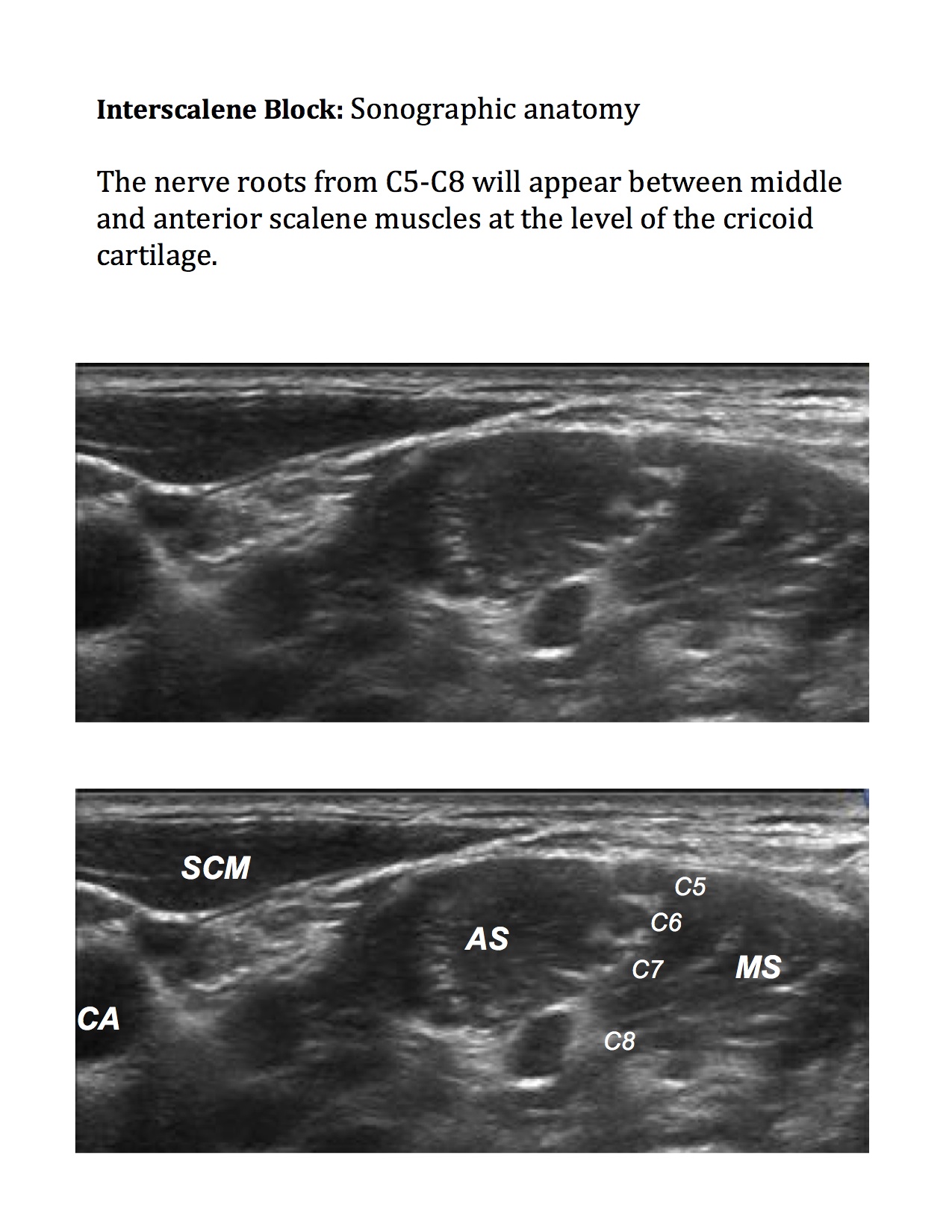
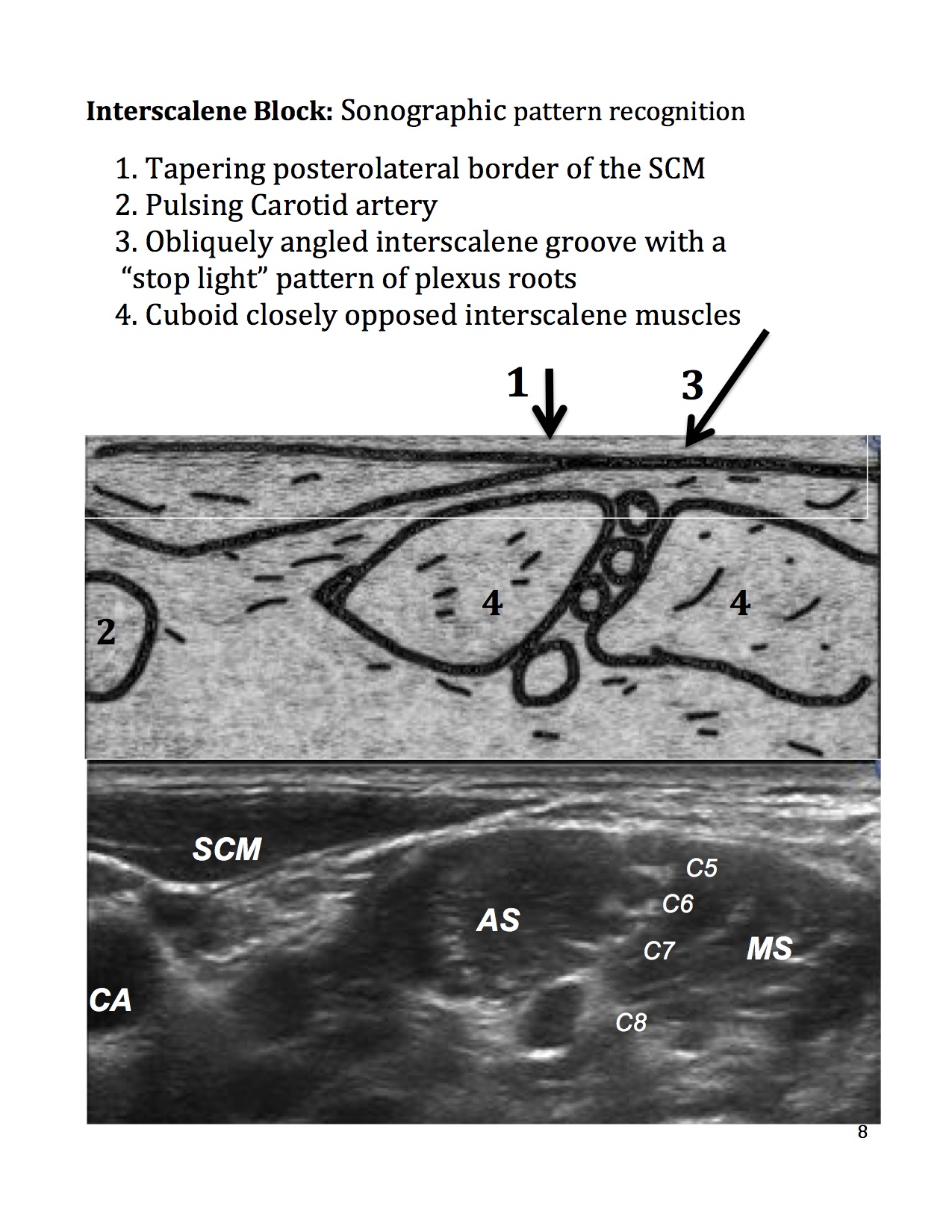
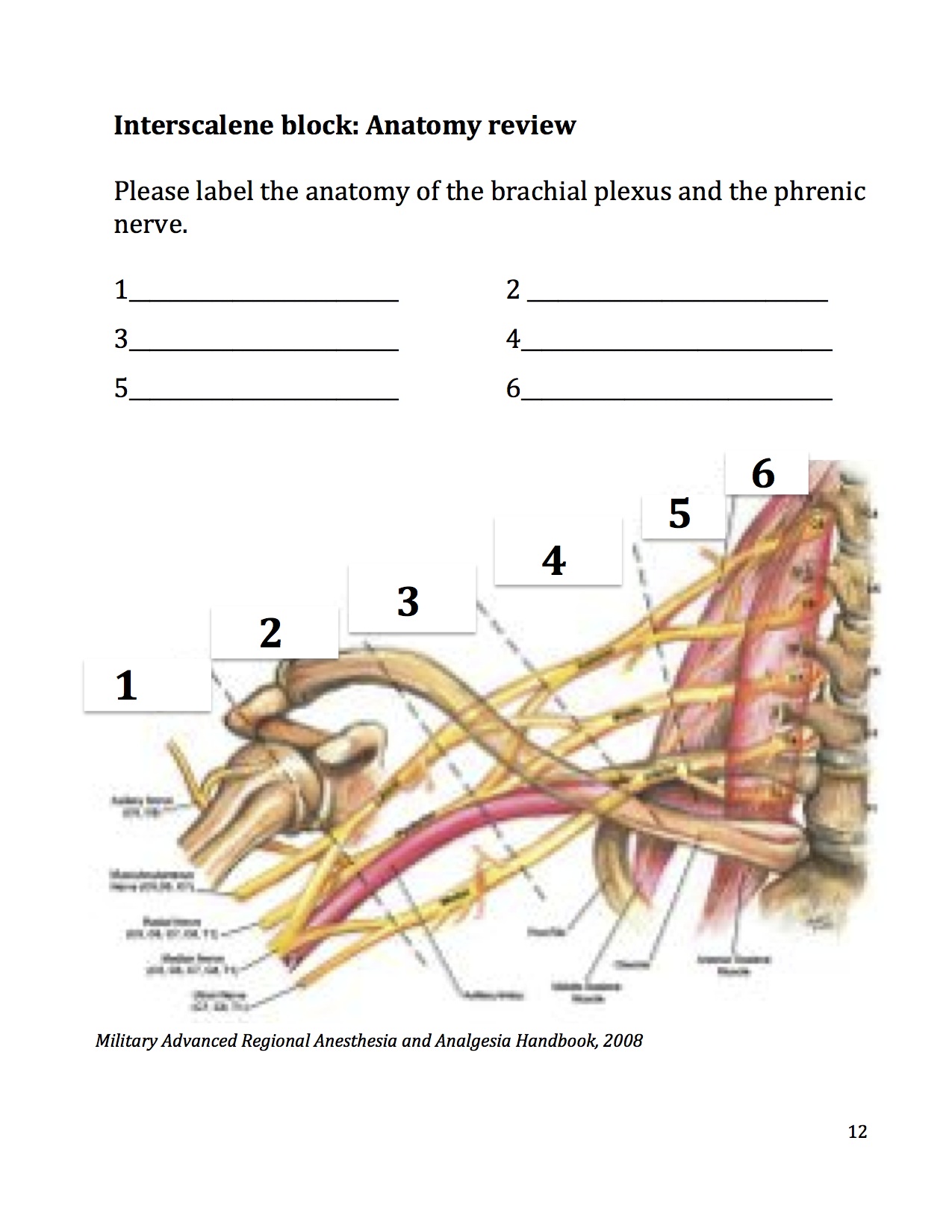
Note that the brachial plexus sits in between the scalene muscles as well as just commonly just under the SCM (sternocleidomastoid muscle). Note the dotted line (prevertebral fascia)

The above ultrasound image should correlate with the drawing above.

The goal is to get the needle tip under the prevertebral fascia and then gently add anesthetic to bathe the brachial plexus.

Make sure to get under the prevetebral fascia


More detailed information below:
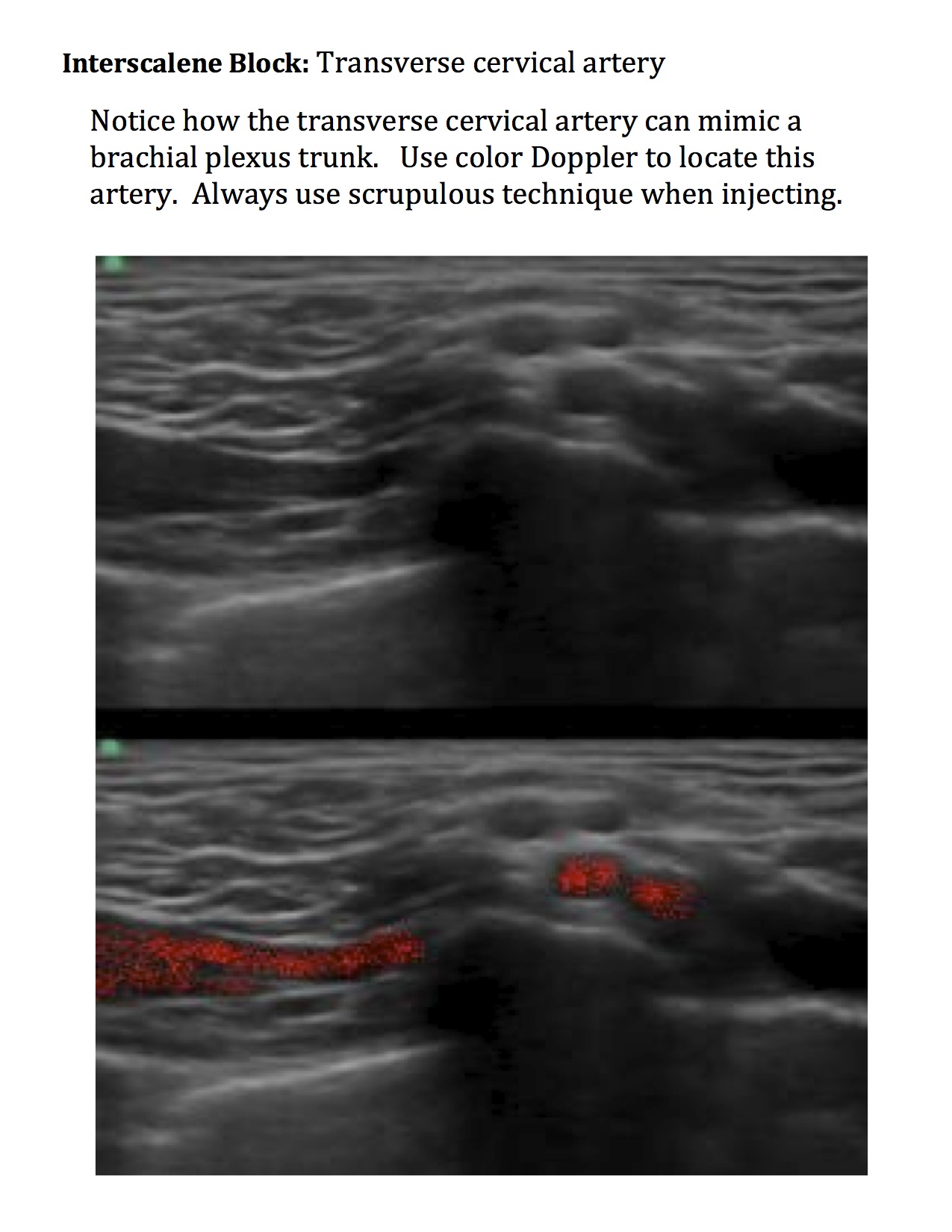
The interscalene block is right up there with the femoral block in regards to its utility in the ED. Overall the neck is a high risk area with lots of vasculature and the nerve roots themselves are relatively vulnerable to needle injury. That said this block is generally very shallow and can be effective with low volumes of local anesthetic. For most shoulder reductions, deltoid I&Ds and proximal humerus fractures a nice block can be placed with 5mL. Check out our curriculum HERE and below. The video is posted HERE.


Out-of-plane interscalene block with the needle tip kept well away from the spinal roots