

Ultrasound-guided block for the medial forearm
/Draining abscesses on the forearm can be a drag, injecting lidocaine into beefy red hot infected tissue hurts, gets messy, and it is easy to get suboptimal anesthesia even after all that stabbing.
Check out full tutorial video HERE

Posterior medial forearm abscess not improving with soaks and warm compresses; patient requesting to have it "opened up."
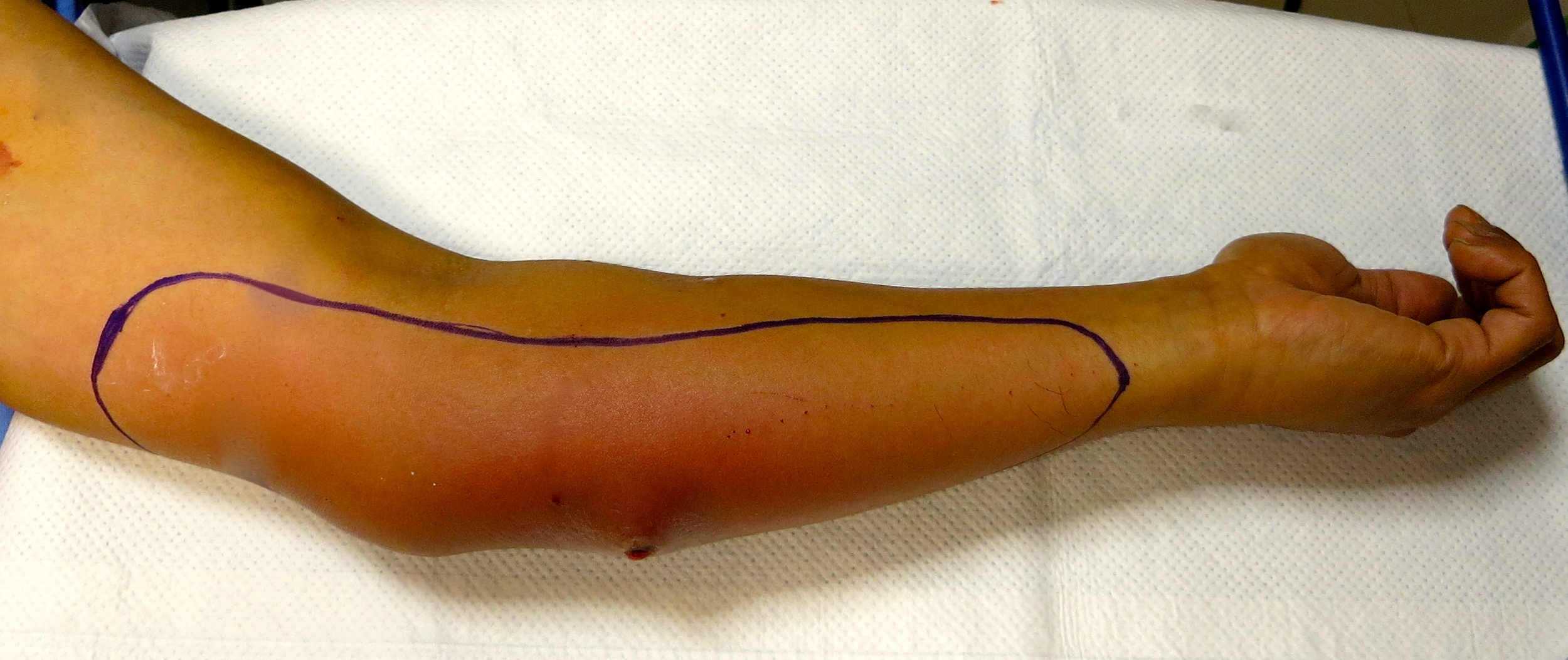
Area of anesthesia after an ultrasound-guided medial antebrachial cutaneous block was placed.

Download quick reference image HERE. The MACN arrises from the C8 and T1 nerve roots and travels within the medial cord. At the axilla it is quite superficial and runs down the medial aspect of the arm as a supeficial nerve in close proximity to the basilic vein. Its branches cover the medial aspect of the arm and forearm. When blocked at the mid-humeral level, the area of anesthesia shown is achieved. An in-plane approach with the arm outstretched is convenient. The nerve itself can be very superficial, its honeycomb appearance allows it to be distinguished from the surrounding connective tissue.

Painless incision and drainage.
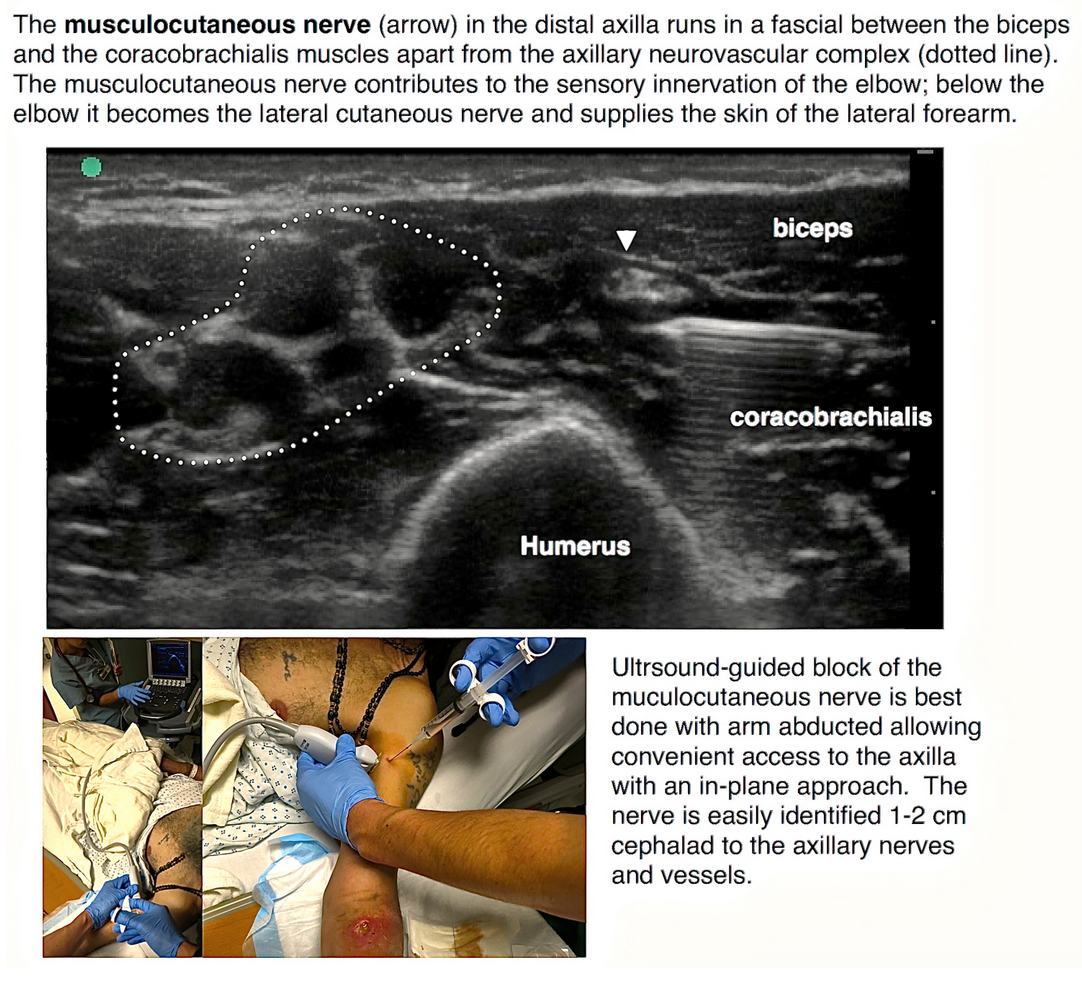
Combine with a musculocutaneous block and you have the entire volar surface of the forearm covered. Remember if an injury is deep, involving the muscle, deep tendons etc...a brachial plexus block is required.

{kind=link}